External Oblique Intercostal Fascial Plane Block
Coauthored with Christopher Ehler

Indications: Anterolateral upper abdominal wall surgery
Special Considerations: The target plane can be very superficial, especially in pediatric patients, and there is limited space between the ribs to drive the needle into the plane deep to the external oblique muscle. Using the ribs as a backstop can reduce the risk of pleural injury.
Patient Position: Supine
Dose: This is a volume-dependent fascial plane block. Please see Local Anesthetic dosing page for ASRA/ESRA suggested dosing guidelines.
Technique: Probe: linear, Needle: In-plane
The probe is placed in the paramedian sagittal plane in between midclavicular and anterior axillary line over the sixth rib. The probe is then rotated slightly with the cranial end rotated towards midline, to view the ribs in short axis. Anatomical structures identified from superficial to deep include subcutaneous tissue, external oblique muscle, intercostal muscles, ribs, pleura, and lungs. The skin is prepped with aseptic solution. An echogenic needle is introduced at cranial end of probe, and advanced in inferolateral direction using in-plane approach. Injection of local anesthetic with frequent aspiration, with spread of local anesthetic visualized in the fascial plane in between external oblique muscle and intercostal muscles and ribs at the level of the sixth rib. A catheter can also be placed into the fascial plane if desired.
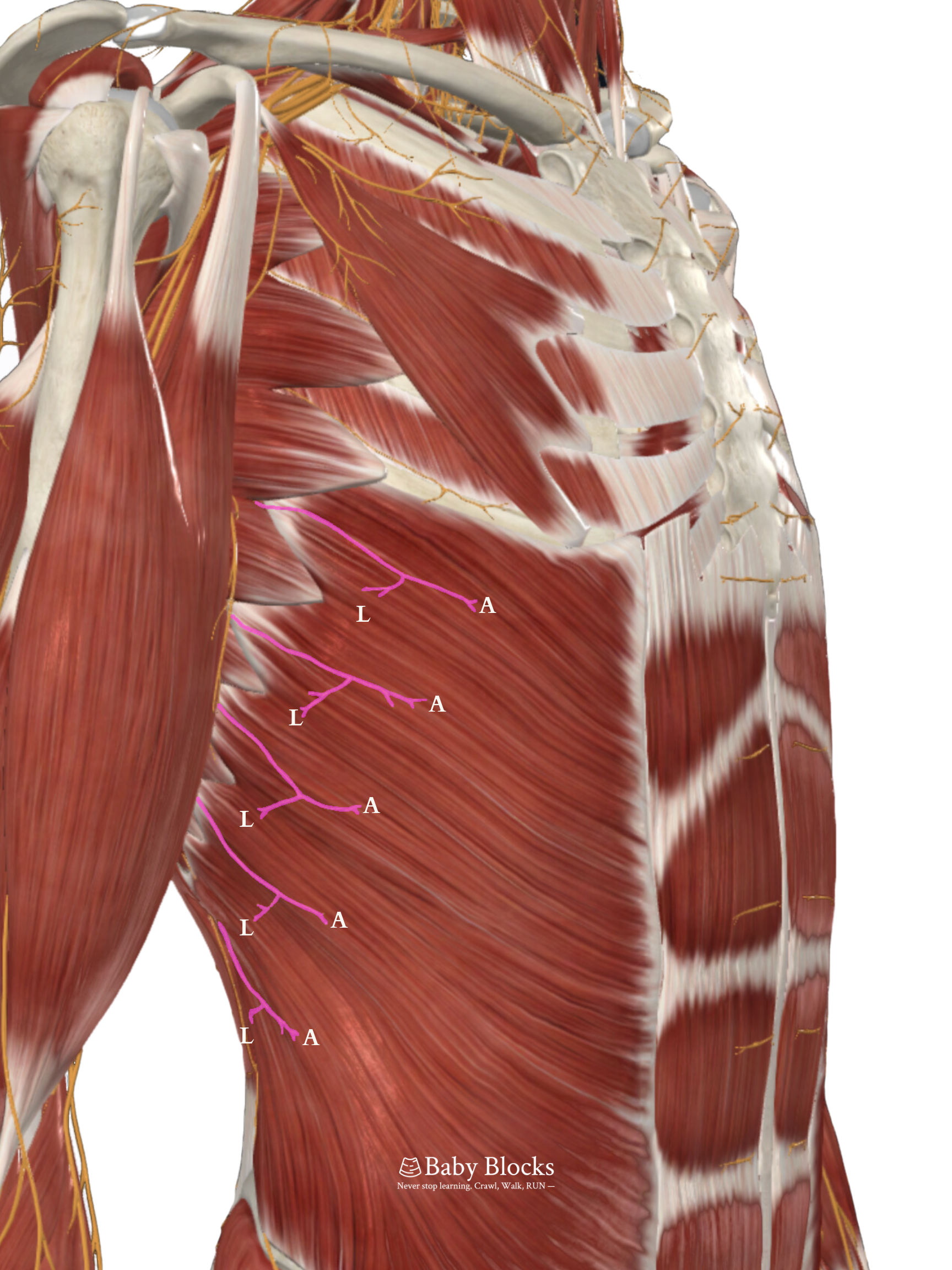
Coverage: Lateral and anterior branches of intercostal nerves from T6 - T10
Potential Complications: site infection, vascular injury, pneumothorax, local anesthetic systemic toxicity

Clinical Pearls: can be performed for upper abdominal surgery, using either single shot technique or catheter insertion for continuous block. If incision crosses the midline, can consider bilateral block.





The external oblique intercostal (EOI) fascial plane block is a relatively new truncal block and provides effective analgesia for upper abdominal surgery. This was first described with a cadaveric study which looked at the spread of dye injected into the fascial plane deep to the external oblique muscle (Hamilton et al., 2019). This proposed analgesic coverage of the intercostal nerves from T6-T10 was then confirmed in the retrospective study by Elsharkawy (Elsharkawy et al., 2021). Many previously-described fascial plane blocks that target the intercostal nerves are able to block either the anterior or lateral branches, but not both without the addition of a second injection. Chen and colleagues were able to demonstrate reliable dermatomal coverage with a subcostal transversus abdominus plane (TAP) block from T7-T12, but with unreliable T6 coverage (Chen et al., 2018). Additionally, the serratus plane block is able to achieve reliable dermatomal coverage from T2-T7, but analgesia below the T7 dermatomal level is less predictable (Hamilton et al., 2019; Blanco et al., 2013). In the EOI cadaveric studies, it was demonstrated that the plane deep to the external oblique muscle is continuous with the tissue plane deep to the serratus anterior. With the EOI block, local anesthetic is able to reach both the lateral and anterior branches of the intercostal nerves from T6 to T10. Therefore, the external oblique fascial plane block is a unique option with sufficient analgesia for many upper abdominal surgeries.
This block targets a dermatomal range appropriate for upper abdominal subcostal or chevron incisions. In the literature, this block has demonstrated benefit for patients undergoing hepatic and biliary tree surgery, living donor nephrectomies, small bowel or colon resections, liver transplants, and many other types of surgery (Elsharkawy et al., 2021; Coşarcan & Erçelen, 2022; Petiz et al., 2023). White and colleagues were able to demonstrate a benefit of the EOI block for patients with obesity undergoing upper abdominal surgery (White & Ji, 2022). One of the limitations of the EOI block is that the caudal end of analgesic coverage ends around T10, and does not reliably cover surgical incisions that extend below the umbilicus. If the incision crosses the midline, bilateral EOI blocks must be performed if analgesic coverage of the entire incision is desired. Additionally, being a fascial plane block, the EOI block will not provide visceral analgesic coverage (Elsharkawy et al., 2021).
While most of the literature regarding the EOI block is written from case reports or case series of adult patients, a literature review showed one case report of this block being performed in a pediatric patient. Wilkinson-Maitland and colleagues present the case of a neonate who underwent Kasai portoenterostomy. Epidural anesthesia was declined, and the patient had bilateral EOI catheters placed for post-operative analgesia. The patient’s airway was extubated at the end of the procedure, and post-operative analgesia was maintained with scheduled hourly intermittent chloroprocaine boluses administered through the EOI catheters. The catheters were removed on post-operative day 5. The authors report post-operative opioid administration for this patient being similar to that for patients who have a continuous epidural catheter placed following Kasai portoenterostomy (Wilkinson-Maitland et al., 2023). The authors also shared technical observations regarding the EOI block in a neonate. Since the tissues overlying the ribs is thin and soft, the angle of approach will be very shallow, almost parallel to the tissue planes. Additionally, there is much less space between the sixth and seventh rib for needle maneuverability in a neonate compared with an adult. Anecdotally, the Baby Blocks editors can confirm that EOI is a useful analgesic modality for pediatric patients undergoing hepatobiliary surgery.
There are many benefits of the EOI block reported in the literature. Understanding the anatomy is often straightforward, and the ribs can be utilized as a backstop for the needle which helps to prevent visceral injury. If the ribs are used as a backstop, care must be taken not to perform an intraosseous injection of local anesthetic, especially if a sharp needle is used. The fascial plane is superficial, which allows it to be compressible if there are concerns of vascular injury or hematoma formation during the procedure. The EOI block is performed with the patient supine, often preventing the need for repositioning. The block provides analgesic coverage of both the anterior and lateral branches of the intercostal nerves ranging across the dermatomes of T6-T10, resulting in analgesia for various upper abdominal surgeries, and requires only 1 injection for unilateral coverage. For patients who would benefit from epidural catheter placement but are unable to receive one due to a contraindication, such as anticoagulation, coagulopathy, patient or caregiver refusal, or spinal pathology, the EOI block serves as an analgesic alternative. It can be performed either as a single shot injection, or with a catheter placed in the plane deep to external oblique for prolonged analgesia. The EOI block has been reported to have a low safety profile, with risks similar to that of an erector spinae plane block (Erskine & White, 2022).
In summary, the external oblique intercostal block is a safe, straightforward fascial plane block with good analgesic coverage for upper abdominal surgery, and has many potential applications for use in pediatric patients.
Hamilton DL, Manickam BP, Wilson MAJ, Abdel Meguid E. External oblique fascial plane block. Reg Anesth Pain Med. 2019 Jan 11:rapm-2018-100256. doi: 10.1136/rapm-2018-100256. Epub ahead of print. PMID: 30635518.
Elsharkawy H, Kolli S, Soliman LM, Seif J, Drake RL, Mariano ER, El-Boghdadly K. The External Oblique Intercostal Block: Anatomic Evaluation and Case Series. Pain Med. 2021 Nov 26;22(11):2436-2442. doi: 10.1093/pm/pnab296. PMID: 34626112.
Chen Y, Shi K, Xia Y, Zhang X, Papadimos TJ, Xu X, Wang Q. Sensory Assessment and Regression Rate of Bilateral Oblique Subcostal Transversus Abdominis Plane Block in Volunteers. Reg Anesth Pain Med. 2018 Feb;43(2):174-179. doi: 10.1097/AAP.0000000000000715. PMID: 29278604.
Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013 Nov;68(11):1107-13. doi: 10.1111/anae.12344. Epub 2013 Aug 7. PMID: 23923989.
Coşarcan SK, Erçelen Ö. The analgesic contribution of external oblique intercostal block: Case reports of 3 different surgeries and 3 spectacular effects. Medicine (Baltimore). 2022 Sep 9;101(36):e30435. doi: 10.1097/MD.0000000000030435. PMID: 36086688.
Petiz C, Barbosa R, Ribeiro Boneco T, Pacheco J, Resende A. External Oblique Intercostal Block for Living Kidney Donor Open Nephrectomy: A Case Series. Cureus. 2023 May 17;15(5):e39139. doi: 10.7759/cureus.39139. PMID: 37332413; PMCID: PMC10275393.
White L, Ji A. External oblique intercostal plane block for upper abdominal surgery: use in obese patients. Br J Anaesth. 2022 May;128(5):e295-e297. doi: 10.1016/j.bja.2022.02.011. Epub 2022 Mar 3. PMID: 35249704.
Wilkinson-Maitland N, Cunningham AJ, Esfahanian M. Postoperative analgesia for Kasai portoenterostomy using external oblique intercostal blocks. Reg Anesth Pain Med. 2023 Dec;48(12):619-621. doi: 10.1136/rapm-2023-104510. Epub 2023 Jul 20. PMID: 37474282.
Erskine RN, White L. "A review of the external oblique intercostal plane block - a novel approach to analgesia for upper abdominal surgery". J Clin Anesth. 2022 Nov;82:110953. doi: 10.1016/j.jclinane.2022.110953. Epub 2022 Aug 19. PMID: 35994942.